Genetic Screening Tests
I recently attended a fascinating talk as part of the South Australian Obstetric Shared Care update by Associate Professor Chris Barnett from the Women’s and Children’s Hospital about the developments in carrier screening and what it means for families. Below are some of those insights. Warning – acronyms aplenty ahead!
The Royal Australian College of Obstetricians and Gynaecologists (RANZOCG) is now recommending that information on carrier screening should be offered to all women planning a pregnancy or in the first trimester of pregnancy. This is not the same as First Trimester Screening (FTS) or Non Invasive Prenatal Testing (NIPT) which is offered to test a fetus for Trisomy 21 (Down Syndrome), Trisomy 18 and in some cases additional chromosomal anomalies. These last two tests are offered in every pregnancy as they are specific for the individual fetus.
Genetic Carrier Screening is a genetic test for an adult, typically done by taking a blood or saliva sample, to determine if a person carries a recessive copy of a gene for specific genetic conditions. The genetic conditions tested for are – Spinal Muscular Atrophy (SMA), Cystic Fibrosis (CF) and Fragile X syndrome (FXS). They are some of the most common inherited recessive conditions in our population and have serious health consequences. A person may be a carrier without knowing and most do not have any family history of these conditions. In order for a person to have this condition, they need to inherit a recessive gene from both parents.
Spinal Muscular Atrophy is a condition that affects nerves and muscles, resulting in weakness, which in turn affects the muscles used to breathe. There are 4 types of SMA, with SMA type 1 being the most common and most severe, with babies affected soon after birth and not usually living beyond 2 years of age. There is currently no cure. For more information on SMA, click here.
Cystic fibrosis is an inherited condition affecting the respiratory and gastrointestinal systems. CF results in thick mucus accumulating in the lungs, trapping bacteria and leading to recurrent chest infections and subsequent lung damage. In the gut, the digestion of food is difficult, leading to inadequate nutrition at times. People with CF often have to take a number of different medications and require multiple hospital admissions usually for infections. Tragically, people with CF have a reduced life expectancy and there is currently no cure, although groundbreaking therapies are currently available for certain mutations. The future looks much brighter for those affected. For more information on CF, click here.
Fragile X Syndrome is the most common cause of inherited intellectual disability. Those affected may have developmental delay, epilepsy, autism and learning and fertility difficulties. Males are more commonly affected than females as they only inherit one X chromosome, often passed down from an asymptomatic mother. There is currently no cure but multidisciplinary teams focus on optimising management. For more information on Fragile X Syndrome, click here.
Genetic Carrier Screening is offered to the pregnant person first. If no recessive mutations are found, then no further testing of the other parent is needed. If it is detected that the pregnant person is a carrier for one of the 3 recessive genetic conditions, then the other biological parent should be screened too. If their test is negative, then the most the baby can be is a carrier.
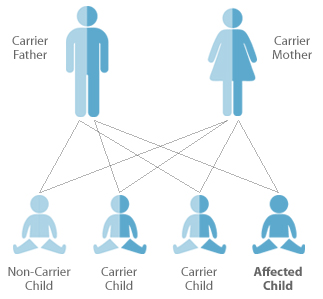
If both parents are carriers their children have a 1 in 4 chance of developing the condition and a 1 in 2 chance of being a carrier for the condition. In the case of Fragile X, male fetuses that inherit the faulty gene from their mother, will have the condition; whereas female fetuses could at most, be a carrier.
An individual has a 1 in 25 chance of being a CF carrier, a 1 in 40 chance of being a SMA carrier and a 1 in 250 chance of being a fragile X carrier. You only need to be tested once in your lifetime (i.e. not with each pregnancy) as your carrier status stays the same. All carriers would be referred to a genetic counselling service for further support and information. Couples may decide to undertake genetic testing of a conceived fetus using chorionic villus sampling (CVS – sample of placental tissue to assess genetic material of the fetus) for a definite diagnosis or to undergo in-vitro fertilization (IVF) with pre-implantation genetic diagnosis to determine if any embryos are affected. Other families may wish to continue a pregnancy regardless but want to know a potential diagnosis before the birth with an amniocentesis (a sample of amniotic fluid is sent off for testing at 15+ weeks of pregnancy). Other options include consideration of using donor egg/sperm/embryo; adoption; or not having children. As with many things, it is a very personal decision.
Genetic carrier screening for cystic fibrosis (CF), spinal muscular atrophy (SMA), and fragile X syndrome (FXS) is now bulk-billed for women who are pregnant or planning pregnancy. Meaning the healthcare provider bills medicare directly and you pay nothing out of pocket for the service. If you are found to be a carrier for CF or SMA, your partner can then be tested for that specific condition to determine your risk as a couple having a child with CF or SMA. The test for each condition is covered once in an individual’s lifetime.
However, it is important to remember that no test guarantees a healthy baby. The screening tests are 90-99% accurate depending on the condition due to the presence of rare genetic mutations in some individuals. There are more extensive panels also available which test for a number of different, less common conditions. These more extensive panels incur additional costs.
As always, our GPs and Midwives are more than happy to discuss all your options during a pre-conception appointment or at one of your first antenatal visits.
More information can be found at:
https://www.vcgs.org.au/tests/prepair
https://www.clinicallabs.com.au/patient/our-tests/pregnancy-testing/gene-access-carrier-screen/
by Dr Rhiannon Smith
Last updated 14/10/2025
Image from: https://globalgenes.org





